What Causes Over-Pronation Of The Foot
Overview
The rolling of the foot is a natural process and the degree to which pronation occurs will depend on an individual?s gait. It has been suggested that up to 70 percent of runners may overpronate to some degree, although it is not always bad for the body even though pronation may not be at optimum levels. Slight overpronation may be perfectly acceptable and may not place an individual at an increased risk of injury; however determining whether this is the case can only come from a doctor, podiatrist or sports therapist. While specialist running shoe stores may be able to spot whether you are an overpronator after observing you on a treadmill and suggest the best running shoes to suit your gait, it is still wise if you are an overpronator to get your gait checked professionally.
Causes
Excess stress on the inner surface of the foot can cause injury and pain in the foot and ankle. Repeated rotational forces through the shin, knee, thigh and pelvis also place additional strain on the muscles, tendons and ligaments of the lower leg.
Symptoms
Overpronation can negatively affect overall body alignment. The lowering of the longitudinal arch pulls the heel bone in, causing the leg, thigh bone and hip to rotate inwards, and an anterior tilt of the pelvis. Unnecessary strain to the ankles, knees, hips and back can result. Plantar fasciitis and inflammation, metatarsal pain, problems with the Achilles tendon, pain on the inside of the knee, and bursitis in the hip are just some of the conditions commonly associated with pronation.
Diagnosis
When sitting, an over-pronating foot appears quite normal, i.e. showing a normal arch with room under the underside of the foot. The moment you get up and put weight on your feet the situation changes: the arches lower and the ankle slightly turns inwards. When you walk or run more weight is placed on the feet compared to standing and over-pronation will become more evident. When walking barefoot on tiles or timber floors over-pronation is more visible, compared to walking on carpet or grass.
Non Surgical Treatment
Personal orthotics can be prescribed via your healthcare professional. If finances or insurance are issues, similar and often better options can be purchased online for overpronation. The right walking shoes are also essential. Most shoes cater to neutral foot gaits, unless they specifically state otherwise. That won?t help you if your foot rolls inward. In order to correct the issue, you need shoes with stability or motion control abilities, low heels, deep heel cups, and good arch support.
Prevention
Custom-made orthotics will reduce the twisting of the leg muscles as they enter the foot, by maintaining a normal alignment of the bones and joints of the foot. If the bones and joints are aligned properly, by reducing the pronation, the muscles can run straight to their attachments in the foot, without twisting to get to these bones. This action of custom-made orthotics will reduce Achilles Tendonitis shin splints; ankle, knee, hip, and lower back pain; and leg cramps. This action will also allow the leg muscles to work more efficiently, thus allowing you to walk and run with less effort.
The rolling of the foot is a natural process and the degree to which pronation occurs will depend on an individual?s gait. It has been suggested that up to 70 percent of runners may overpronate to some degree, although it is not always bad for the body even though pronation may not be at optimum levels. Slight overpronation may be perfectly acceptable and may not place an individual at an increased risk of injury; however determining whether this is the case can only come from a doctor, podiatrist or sports therapist. While specialist running shoe stores may be able to spot whether you are an overpronator after observing you on a treadmill and suggest the best running shoes to suit your gait, it is still wise if you are an overpronator to get your gait checked professionally.
Causes
Excess stress on the inner surface of the foot can cause injury and pain in the foot and ankle. Repeated rotational forces through the shin, knee, thigh and pelvis also place additional strain on the muscles, tendons and ligaments of the lower leg.
Symptoms
Overpronation can negatively affect overall body alignment. The lowering of the longitudinal arch pulls the heel bone in, causing the leg, thigh bone and hip to rotate inwards, and an anterior tilt of the pelvis. Unnecessary strain to the ankles, knees, hips and back can result. Plantar fasciitis and inflammation, metatarsal pain, problems with the Achilles tendon, pain on the inside of the knee, and bursitis in the hip are just some of the conditions commonly associated with pronation.
Diagnosis
When sitting, an over-pronating foot appears quite normal, i.e. showing a normal arch with room under the underside of the foot. The moment you get up and put weight on your feet the situation changes: the arches lower and the ankle slightly turns inwards. When you walk or run more weight is placed on the feet compared to standing and over-pronation will become more evident. When walking barefoot on tiles or timber floors over-pronation is more visible, compared to walking on carpet or grass.
Non Surgical Treatment
Personal orthotics can be prescribed via your healthcare professional. If finances or insurance are issues, similar and often better options can be purchased online for overpronation. The right walking shoes are also essential. Most shoes cater to neutral foot gaits, unless they specifically state otherwise. That won?t help you if your foot rolls inward. In order to correct the issue, you need shoes with stability or motion control abilities, low heels, deep heel cups, and good arch support.
Prevention
Custom-made orthotics will reduce the twisting of the leg muscles as they enter the foot, by maintaining a normal alignment of the bones and joints of the foot. If the bones and joints are aligned properly, by reducing the pronation, the muscles can run straight to their attachments in the foot, without twisting to get to these bones. This action of custom-made orthotics will reduce Achilles Tendonitis shin splints; ankle, knee, hip, and lower back pain; and leg cramps. This action will also allow the leg muscles to work more efficiently, thus allowing you to walk and run with less effort.
What Exactly Is Severs Disease?
Overview
Severs disease is pain in one or both heels when walking. The pain comes from the area between the sections of bone that make up the heel. As you go through a ?growth spurt? the tendon at the back of the heel (Achilles tendon) pulls at the heel bone. This makes you limp or walk on your toes and often creates a lump on your heel. The reason the tendon is tight is because your bones grow faster than your muscles. It usually affects boys between eight to ten years old, girls between ten and 12 years old, children in a ?growth spurt?, children involved in sports, usually those that involve running and jumping.
Causes
The usual cause is directly related to overuse of the bone and tendons in the heel. This can come from playing sports or anything that involves a lot of heel movement. It can be associated with starting a new sport, or the start of a new season, or too much weight bearing on the heel. Also, excessive traction could cause this, since the bones and tendons are still developing. Many children who over pronate their feet exhibit symptoms and in most patients, it usually involves both heels.
Symptoms
The typical patient is a child between 10 and 13 years of age, complaining of pain in one or both heels with running and walking. The pain is localized to the point of the heel where the tendo-Achilles inserts into the calcaneus, and is tender to deep pressure at that site. Walking on his toes relieves the pain.
Diagnosis
Sever?s disease is diagnosed based on a doctor?s physical examination of the lower leg, ankle, and foot. If the diagnosis is in question, the doctor may order x-rays or an MRI to determine if there are other injuries that may be causing the heel pain.
Non Surgical Treatment
The physiotherapist will thoroughly assess the affected areas and general mechanics to determine what factors may be contributing, also to rule out any other injuries or stress fractures, etc. Treatment focusing on the affected area will consist of modified rest, ice, massage, stretches and electrotherapy. A foam heel raise may also be given to help decrease pain. The physiotherapist may also treat other areas if biomechanical problems are noted. This may include massage, mobilization and exercises to stretch and strengthen certain areas. They may also refer the patient to see a podiatrist if they believe the foot posture is a factor.
Severs disease is pain in one or both heels when walking. The pain comes from the area between the sections of bone that make up the heel. As you go through a ?growth spurt? the tendon at the back of the heel (Achilles tendon) pulls at the heel bone. This makes you limp or walk on your toes and often creates a lump on your heel. The reason the tendon is tight is because your bones grow faster than your muscles. It usually affects boys between eight to ten years old, girls between ten and 12 years old, children in a ?growth spurt?, children involved in sports, usually those that involve running and jumping.
Causes
The usual cause is directly related to overuse of the bone and tendons in the heel. This can come from playing sports or anything that involves a lot of heel movement. It can be associated with starting a new sport, or the start of a new season, or too much weight bearing on the heel. Also, excessive traction could cause this, since the bones and tendons are still developing. Many children who over pronate their feet exhibit symptoms and in most patients, it usually involves both heels.
Symptoms
The typical patient is a child between 10 and 13 years of age, complaining of pain in one or both heels with running and walking. The pain is localized to the point of the heel where the tendo-Achilles inserts into the calcaneus, and is tender to deep pressure at that site. Walking on his toes relieves the pain.
Diagnosis
Sever?s disease is diagnosed based on a doctor?s physical examination of the lower leg, ankle, and foot. If the diagnosis is in question, the doctor may order x-rays or an MRI to determine if there are other injuries that may be causing the heel pain.
Non Surgical Treatment
The physiotherapist will thoroughly assess the affected areas and general mechanics to determine what factors may be contributing, also to rule out any other injuries or stress fractures, etc. Treatment focusing on the affected area will consist of modified rest, ice, massage, stretches and electrotherapy. A foam heel raise may also be given to help decrease pain. The physiotherapist may also treat other areas if biomechanical problems are noted. This may include massage, mobilization and exercises to stretch and strengthen certain areas. They may also refer the patient to see a podiatrist if they believe the foot posture is a factor.
How To Cure Flat Feet In Adults
Overview
Adult flatfoot may be due to multiple problems including a dysfunctional posterior tibial tendon (PTT), hypermobility and ligamentous laxity, or possibly a coalition that becomes symptomatic. For a vast majority of patients, posterior tibial tendon dysfunction (PTTD) is the cause of symptomatic flatfoot and is the main trigger of surgical reconstruction in flatfoot. The common presenting scenario for adult flatfoot is a case of unilateral flatfoot with pain. Patients will often confirm they ?always had flat feet? but have noticed increased pain and additional collapse in the past few months to years. They may also note increased swelling and a possible concern over one foot increasing in shoe size. After a comprehensive dermatologic, neurologic and vascular assessment, one should direct his or her attention to the musculoskeletal portion of the exam. It is key to examine the foot and leg as a whole in order to determine the proper procedure and consider each phase of the corrective surgery. 
Causes
As the name suggests, adult-acquired flatfoot occurs once musculoskeletal maturity is reached, and it can present for a number of reasons, though one stands out among the others. While fractures, dislocations, tendon lacerations, and other such traumatic events do contribute to adult-acquired flatfoot as a significant lower extremity disorder, as mentioned above, damage to the posterior tibial tendon is most often at the heart of adult-acquired flatfoot. One study further elaborates on the matter by concluding that ?60% of patients [presenting with posterior tibial tendon damage and adult-acquired flatfoot] were obese or had diabetes mellitus, hypertension, previous surgery or trauma to the medial foot, or treatment with steroids?.
Symptoms
Symptoms shift around a bit, depending on what stage of PTTD you?re in. For instance, you?re likely to start off with tendonitis, or inflammation of the posterior tibial tendon. This will make the area around the inside of your ankle and possibly into your arch swollen, reddened, warm to the touch, and painful. Inflammation may actually last throughout the stages of PTTD. The ankle will also begin to roll towards the inside of the foot (pronate), your heel may tilt, and you may experience some pain in your leg (e.g. shin splints). As the condition progresses, the toes and foot begin to turn outward, so that when you look at your foot from the back (or have a friend look for you, because-hey-that can be kind of a difficult maneuver to pull off) more toes than usual will be visible on the outside (i.e. the side with the pinky toe). At this stage, the foot?s still going to be flexible, although it will likely have flattened somewhat due to the lack of support from the posterior tibial tendon. You may also find it difficult to stand on your toes. Finally, you may reach a stage in which your feet are inflexibly flat. At this point, you may experience pain below your ankle on the outside of your foot, and you might even develop arthritis in the ankle.
Diagnosis
In the early stages of dysfunction of the posterior tibial tendon, most of the discomfort is located medially along the course of the tendon and the patient reports fatigue and aching on the plantar-medial aspect of the foot and ankle. Swelling is common if the dysfunction is associated with tenosynovitis. As dysfunction of the tendon progresses, maximum pain occurs laterally in the sinus tarsi because of impingement of the fibula against the calcaneus. With increasing deformity, patients report that the shape of the foot changes and that it becomes increasingly difficult to wear shoes. Many patients no longer report pain in the medial part of the foot and ankle after a complete rupture of the posterior tibial tendon has occurred; instead, the pain is located laterally. If a fixed deformity has not occurred, the patient may report that standing or walking with the hindfoot slightly inverted alleviates the lateral impingement and relieves the pain in the lateral part of the foot.
Non surgical Treatment
Medical or nonoperative therapy for posterior tibial tendon dysfunction involves rest, immobilization, nonsteroidal anti-inflammatory medication, physical therapy, orthotics, and bracing. This treatment is especially attractive for patients who are elderly, who place low demands on the tendon, and who may have underlying medical problems that preclude operative intervention. During stage 1 posterior tibial tendon dysfunction, pain, rather than deformity, predominates. Cast immobilization is indicated for acute tenosynovitis of the posterior tibial tendon or for patients whose main presenting feature is chronic pain along the tendon sheath. A well-molded short leg walking cast or removable cast boot should be used for 6-8 weeks. Weight bearing is permitted if the patient is able to ambulate without pain. If improvement is noted, the patient then may be placed in custom full-length semirigid orthotics. The patient may then be referred to physical therapy for stretching of the Achilles tendon and strengthening of the posterior tibial tendon. Steroid injection into the posterior tibial tendon sheath is not recommended due to the possibility of causing a tendon rupture. In stage 2 dysfunction, a painful flexible deformity develops, and more control of hindfoot motion is required. In these cases, a rigid University of California at Berkley (UCBL) orthosis or short articulated ankle-foot orthosis (AFO) is indicated. Once a rigid flatfoot deformity develops, as in stage 3 or 4, bracing is extended above the ankle with a molded AFO, double upright brace, or patellar-tendon-bearing brace. The goals of this treatment are to accommodate the deformity, prevent or slow further collapse, and improve walking ability by transferring load to the proximal leg away from the collapsed medial midfoot and heel. 
Surgical Treatment
Good to excellent results for more than 80% of patients have been reported at five years' follow up for the surgical interventions recommended below. However, the postoperative recovery is a lengthy process, and most surgical procedures require patients to wear a plaster cast for two to three months. Although many patients report that their function is well improved by six months, in our experience a year is required to recover truly and gain full functional improvement after the surgery. Clearly, some patients are not candidates for such major reconstructive surgery.
Flat Feet In Adults
Overview
Adult Acquired Flatfoot (Posterior Tibial Tendon Dysfunction) is a painful, progressive deformity in adults. It results from a gradual stretch (attenuation) of the tibialis posterior tendon and the ligaments that support your foot's arch. This stretching causes the tendon to lose strength and function. Many people have flat feet and do not experience pain. However, pain occurs with Adult Acquired Flatfoot because the tendons and ligaments have been torn. Once the vital ligaments and posterior tibial tendon are lost, there is no longer anything holding the arch of the foot in place.
Causes
Posterior tibial tendon dysfunction is the most common cause of acquired adult flatfoot deformity. There is often no specific event that starts the problem, such as a sudden tendon injury. More commonly, the tendon becomes injured from cumulative wear and tear. Posterior tibial tendon dysfunction occurs more commonly in patients who already have a flat foot for other reasons. As the arch flattens, more stress is placed on the posterior tibial tendon and also on the ligaments on the inside of the foot and ankle. The result is a progressive disorder.
Symptoms
The types of symptoms that may indicate Adult-Acquired Flat Foot Deformity include foot pain that worsens over time, loss of the arch, abnormal shoe wear (excessive wearing on the inner side of shoe from walking on the inner side of the foot) and an awkward appearance of the foot and ankle (when viewed from behind, heel and toes appear to go out to the side). It is important that we help individuals recognize the early symptoms of this condition, as there are many treatment options, depending upon the severity, the age of the patient, and the desired activity levels.
Diagnosis
Observe forefoot to hindfoot alignment. Do this with the patient sitting and the heel in neutral, and also with the patient standing. I like to put blocks under the forefoot with the heel in neutral to see how much forefoot correction is necessary to help hold the hindfoot position. One last note is to check all joints for stiffness. In cases of prolonged PTTD or coalition, rigid deformity is present and one must carefully check the joints of the midfoot and hindfoot for stiffness and arthritis in the surgical pre-planning.
Non surgical Treatment
Initial treatment for most patients consists of rest and anti-inflammatory medications. This will help reduce the swelling and pain associated with the condition. The long term treatment for the problem usually involves custom made orthotics and supportive shoe gear to prevent further breakdown of the foot. ESWT(extracorporeal shock wave therapy) is a novel treatment which uses sound wave technology to stimulate blood flow to the tendon to accelerate the healing process. This can help lead to a more rapid return to normal activities for most patients. If treatment is initiated early in the process, most patients can experience a return to normal activities without the need for surgery.

Surgical Treatment
If cast immobilization fails, surgery is the next alternative. Treatment goals include eliminating pain, halting deformity progression and improving mobility. Subtalar Arthroereisis, 15 minute outpatient procedure, may correct flexible flatfoot deformity (hyperpronation). The procedure involves placing an implant under the ankle joint (sinus tarsi) to prevent abnormal motion. Very little recovery time is required and it is completely reversible if necessary. Ask your Dallas foot doctor for more information about this exciting treatment possibility.
Adult Acquired Flatfoot (Posterior Tibial Tendon Dysfunction) is a painful, progressive deformity in adults. It results from a gradual stretch (attenuation) of the tibialis posterior tendon and the ligaments that support your foot's arch. This stretching causes the tendon to lose strength and function. Many people have flat feet and do not experience pain. However, pain occurs with Adult Acquired Flatfoot because the tendons and ligaments have been torn. Once the vital ligaments and posterior tibial tendon are lost, there is no longer anything holding the arch of the foot in place.
Causes
Posterior tibial tendon dysfunction is the most common cause of acquired adult flatfoot deformity. There is often no specific event that starts the problem, such as a sudden tendon injury. More commonly, the tendon becomes injured from cumulative wear and tear. Posterior tibial tendon dysfunction occurs more commonly in patients who already have a flat foot for other reasons. As the arch flattens, more stress is placed on the posterior tibial tendon and also on the ligaments on the inside of the foot and ankle. The result is a progressive disorder.
Symptoms
The types of symptoms that may indicate Adult-Acquired Flat Foot Deformity include foot pain that worsens over time, loss of the arch, abnormal shoe wear (excessive wearing on the inner side of shoe from walking on the inner side of the foot) and an awkward appearance of the foot and ankle (when viewed from behind, heel and toes appear to go out to the side). It is important that we help individuals recognize the early symptoms of this condition, as there are many treatment options, depending upon the severity, the age of the patient, and the desired activity levels.
Diagnosis
Observe forefoot to hindfoot alignment. Do this with the patient sitting and the heel in neutral, and also with the patient standing. I like to put blocks under the forefoot with the heel in neutral to see how much forefoot correction is necessary to help hold the hindfoot position. One last note is to check all joints for stiffness. In cases of prolonged PTTD or coalition, rigid deformity is present and one must carefully check the joints of the midfoot and hindfoot for stiffness and arthritis in the surgical pre-planning.
Non surgical Treatment
Initial treatment for most patients consists of rest and anti-inflammatory medications. This will help reduce the swelling and pain associated with the condition. The long term treatment for the problem usually involves custom made orthotics and supportive shoe gear to prevent further breakdown of the foot. ESWT(extracorporeal shock wave therapy) is a novel treatment which uses sound wave technology to stimulate blood flow to the tendon to accelerate the healing process. This can help lead to a more rapid return to normal activities for most patients. If treatment is initiated early in the process, most patients can experience a return to normal activities without the need for surgery.
Surgical Treatment
If cast immobilization fails, surgery is the next alternative. Treatment goals include eliminating pain, halting deformity progression and improving mobility. Subtalar Arthroereisis, 15 minute outpatient procedure, may correct flexible flatfoot deformity (hyperpronation). The procedure involves placing an implant under the ankle joint (sinus tarsi) to prevent abnormal motion. Very little recovery time is required and it is completely reversible if necessary. Ask your Dallas foot doctor for more information about this exciting treatment possibility.
What Are The Most Obvious Principal Treatment And Cause Of Achilles Tendon Pain ?
Overview
 If you have pain along the back of your leg near your heel, you may have Achilles tendonitis. Achilles tendonitis is an overuse injury that commonly occurs in runners and ?weekend warriors?. The Achilles tendon is the largest tendon in the body. Named after a tragic hero from Greek mythology, it connects your calf muscle to your heel bone to allow you to jump, run and walk. Achilles tendonitis is most common in middle-aged men, but it can happen to anyone who has a sudden increase in physical activity. The risk is increased if you also have tight calf muscles and/or a flat arch in your foot. Other risk factors include running in worn out shoes, cold weather, frequently running uphill or if you suffer from medical conditions such as diabetes or high blood pressure. There are two main types of Achilles tendinitis: insertional and noninsertional. Insertional Achilles tendinitis involves the lower portion of the heel, where the tendon attaches to the heel bone. Noninsertional Achilles tendinitis is when the fibers in the middle portion of the tendon have started to break down with tiny tears, swell, and/or thicken. This type is more often seen in younger, active people. Both types can also cause bone spurs. Achilles tendonitis should be diagnosed by your doctor. However, if you experienced a sudden ?pop? in the back of your calf or heel, this might be something more serious like a ruptured or torn Achilles tendon. If this happens, see your doctor immediately.
If you have pain along the back of your leg near your heel, you may have Achilles tendonitis. Achilles tendonitis is an overuse injury that commonly occurs in runners and ?weekend warriors?. The Achilles tendon is the largest tendon in the body. Named after a tragic hero from Greek mythology, it connects your calf muscle to your heel bone to allow you to jump, run and walk. Achilles tendonitis is most common in middle-aged men, but it can happen to anyone who has a sudden increase in physical activity. The risk is increased if you also have tight calf muscles and/or a flat arch in your foot. Other risk factors include running in worn out shoes, cold weather, frequently running uphill or if you suffer from medical conditions such as diabetes or high blood pressure. There are two main types of Achilles tendinitis: insertional and noninsertional. Insertional Achilles tendinitis involves the lower portion of the heel, where the tendon attaches to the heel bone. Noninsertional Achilles tendinitis is when the fibers in the middle portion of the tendon have started to break down with tiny tears, swell, and/or thicken. This type is more often seen in younger, active people. Both types can also cause bone spurs. Achilles tendonitis should be diagnosed by your doctor. However, if you experienced a sudden ?pop? in the back of your calf or heel, this might be something more serious like a ruptured or torn Achilles tendon. If this happens, see your doctor immediately.
Causes
Tendons are the tough fibres that connect muscle to bone. Most tendon injuries occur near joints, such as the shoulder, elbow, knee, and ankle. A tendon injury may seem to happen suddenly, but usually it is the result of many tiny tears to the tendon that have happened over time. Health professionals may use different terms to describe a tendon injury. You may hear, Tendonitis (or Tendinitis): This actually means "inflammation of the tendon," but inflammation is rarely the cause of your tendon pain.
Symptoms
A symptom is something the patient feels and reports, while a sign is something other people, such as a doctor, detect. For example, pain is a symptom, while a rash is a sign. The most typical symptom of Achilles tendinitis is a gradual buildup of pain that deteriorates with time. With Achilles tendinitis, the Achilles tendon may feel sore a few centimeters above where it meets the heel bone. Other possible signs and symptoms of Achilles tendinitis are, the Achilles tendon feels sore a few centimeters above where it meets the heel bone, lower leg feels stiff or lower leg feels slow and weak. Slight pain in the back of the leg that appears after running or exercising, and worsens, pain in the Achilles tendon that occurs while running or a couple of hours afterwards. Greater pain experienced when running fast (such as sprinting), for a long time (such as cross country), or even when climbing stairs. The Achilles tendon swells or forms a bump or the Achilles tendon creaks when touched or moved. Please note that these symptoms, and others similar can occur in other conditions, so for an accurate diagnosis, the patient would need to visit their doctor.
Diagnosis
If Achilles tendonitis is suspected, avoid any exercise or activity that causes the pain. It is advisable to see a doctor promptly so that an accurate diagnosis can be made and appropriate treatment recommended. The doctor will take a full medical history and will ask about the nature and duration of the symptoms. They will perform a physical examination of the affected area. Ultrasound scanning may be used to assess damage to the tendon or surrounding structures. Occasionally MRI (magnetic resonance imaging) may be recommended. The symptoms of Achilles tendonitis are often similar to symptoms of other conditions such as partial Achilles tendon rupture and heel bursitis. This can make diagnosis difficult and a referral to an orthopaedic specialist may be required in order for an accurate diagnosis to be made.
Nonsurgical Treatment
The aim, when treating Achilles tendinitis, is to relieve pain and reduce swelling. The kind of treatment used can vary, based on the severity of the condition and whether or not the patient is a professional athlete. After diagnosis, the doctor will decide which method of treatment is required for the patient to undergo, it is likely that they will suggest a combination. Stretching achilles tendon, a doctor might show the patient some stretching exercises that help the Achilles tendon heal, as well as preventing future injury. Methods used to treat Achilles tendinitis include, ice packs - applying these to the tendon, when in pain or after exercising, can alleviate the pain and inflammation. Resting, this gives the tissue time to heal. The type of rest needed depends on the severity of the symptoms. In mild cases of Achilles tendinitis, it may mean just reducing the intensity of a workout, in severe cases it might mean complete rest for days or weeks. Elevating the foot, swelling can be reduced if the foot is kept raised above the level of the heart. Exercise and stretching, a doctor might show the patient some stretching exercises that help the Achilles tendon heal, as well as preventing future injury. They may, instead, refer the patient to a physiotherapist or another specialist. The exercises learned will improve the flexibility of the area and likely increase calf strength. Pain relievers - non-steroidal anti-inflammatory drugs (NSAIDS), such as ibuprofen can reduce pain and swelling. If you suffer from asthma, kidney disease or liver disease do not take NSAIDs without first checking with your doctor. Steroid injections, these can reduce tendon swelling, but should be performed with caution, as this process has been associated with a greater risk of tendon rupture. A doctor would likely perform the injection while scanning the area with ultrasound to reduce this risk. Compression bandages and orthotic devices, such as ankle supports and shoe inserts can aid recovery as they take the stress off the Achilles tendon.

Surgical Treatment
Percutaneous Achilles Tendon Surgery. During this procedure the surgeon will make 3 to 4 incisions (approx. 2.5 cm long) on both sides of the Achilles tendon. Small forceps are used to free the tendon sheath (the soft tissue casing around your Achilles tendon) to make room for the surgeon to stitch/suture any tears. Skilled surgeons may perform a percutaneous achilles tendon surgery with ultrasound imaging techniques to allow for blink suturing with stab incisions made by a surgical suture needle. This procedure can be done in 3 different ways depending on the preference and experience of your surgeon. Instead of making several 2.5 cm incisions for this procedure, some surgeons will use guided imaging with an ultrasound to see the Achilles tendon tissue without having to open up your ankle. For this technique, they will use a surgical needle to repeatedly stab your Achilles tendon. These "stab incisions" will allow the surgeon to "blindly" suture your tendon without seeing the actual tissue. As another option - some surgeons will only make 1 to 3 incisions for smaller surgical implements to repair your tendon while relying on imaging ultrasound to see your damaged tissue. During either procedure the use of ultrasound imaging or endoscopic techniques requires a very skilled surgeon.
Prevention
By properly training the body, an athlete can build the strength of their tendons and muscles. Following a workout and dieting plan, the body will be able to build muscle and strengthen most effectively. Additionally, doing the following can prevent tendinitis. Wearing appropriate shoes will give your foot the support it needs for proper movements of the foot and ankle. Improper movements will put additional stress on your body. Stretching before an athletic activity, Stretching primes the body for a taxing activity. Additionally, this will get your blood flowing and reduce the risk of pulling a muscle. Ask your doctor about orthotics, Custom orthotics can help get your foot into proper alignment. If the foot does not execute proper mechanics, the body will adjust which will cause pain and increase the chances of injury.
If you have pain along the back of your leg near your heel, you may have Achilles tendonitis. Achilles tendonitis is an overuse injury that commonly occurs in runners and ?weekend warriors?. The Achilles tendon is the largest tendon in the body. Named after a tragic hero from Greek mythology, it connects your calf muscle to your heel bone to allow you to jump, run and walk. Achilles tendonitis is most common in middle-aged men, but it can happen to anyone who has a sudden increase in physical activity. The risk is increased if you also have tight calf muscles and/or a flat arch in your foot. Other risk factors include running in worn out shoes, cold weather, frequently running uphill or if you suffer from medical conditions such as diabetes or high blood pressure. There are two main types of Achilles tendinitis: insertional and noninsertional. Insertional Achilles tendinitis involves the lower portion of the heel, where the tendon attaches to the heel bone. Noninsertional Achilles tendinitis is when the fibers in the middle portion of the tendon have started to break down with tiny tears, swell, and/or thicken. This type is more often seen in younger, active people. Both types can also cause bone spurs. Achilles tendonitis should be diagnosed by your doctor. However, if you experienced a sudden ?pop? in the back of your calf or heel, this might be something more serious like a ruptured or torn Achilles tendon. If this happens, see your doctor immediately.
Causes
Tendons are the tough fibres that connect muscle to bone. Most tendon injuries occur near joints, such as the shoulder, elbow, knee, and ankle. A tendon injury may seem to happen suddenly, but usually it is the result of many tiny tears to the tendon that have happened over time. Health professionals may use different terms to describe a tendon injury. You may hear, Tendonitis (or Tendinitis): This actually means "inflammation of the tendon," but inflammation is rarely the cause of your tendon pain.
Symptoms
A symptom is something the patient feels and reports, while a sign is something other people, such as a doctor, detect. For example, pain is a symptom, while a rash is a sign. The most typical symptom of Achilles tendinitis is a gradual buildup of pain that deteriorates with time. With Achilles tendinitis, the Achilles tendon may feel sore a few centimeters above where it meets the heel bone. Other possible signs and symptoms of Achilles tendinitis are, the Achilles tendon feels sore a few centimeters above where it meets the heel bone, lower leg feels stiff or lower leg feels slow and weak. Slight pain in the back of the leg that appears after running or exercising, and worsens, pain in the Achilles tendon that occurs while running or a couple of hours afterwards. Greater pain experienced when running fast (such as sprinting), for a long time (such as cross country), or even when climbing stairs. The Achilles tendon swells or forms a bump or the Achilles tendon creaks when touched or moved. Please note that these symptoms, and others similar can occur in other conditions, so for an accurate diagnosis, the patient would need to visit their doctor.
Diagnosis
If Achilles tendonitis is suspected, avoid any exercise or activity that causes the pain. It is advisable to see a doctor promptly so that an accurate diagnosis can be made and appropriate treatment recommended. The doctor will take a full medical history and will ask about the nature and duration of the symptoms. They will perform a physical examination of the affected area. Ultrasound scanning may be used to assess damage to the tendon or surrounding structures. Occasionally MRI (magnetic resonance imaging) may be recommended. The symptoms of Achilles tendonitis are often similar to symptoms of other conditions such as partial Achilles tendon rupture and heel bursitis. This can make diagnosis difficult and a referral to an orthopaedic specialist may be required in order for an accurate diagnosis to be made.
Nonsurgical Treatment
The aim, when treating Achilles tendinitis, is to relieve pain and reduce swelling. The kind of treatment used can vary, based on the severity of the condition and whether or not the patient is a professional athlete. After diagnosis, the doctor will decide which method of treatment is required for the patient to undergo, it is likely that they will suggest a combination. Stretching achilles tendon, a doctor might show the patient some stretching exercises that help the Achilles tendon heal, as well as preventing future injury. Methods used to treat Achilles tendinitis include, ice packs - applying these to the tendon, when in pain or after exercising, can alleviate the pain and inflammation. Resting, this gives the tissue time to heal. The type of rest needed depends on the severity of the symptoms. In mild cases of Achilles tendinitis, it may mean just reducing the intensity of a workout, in severe cases it might mean complete rest for days or weeks. Elevating the foot, swelling can be reduced if the foot is kept raised above the level of the heart. Exercise and stretching, a doctor might show the patient some stretching exercises that help the Achilles tendon heal, as well as preventing future injury. They may, instead, refer the patient to a physiotherapist or another specialist. The exercises learned will improve the flexibility of the area and likely increase calf strength. Pain relievers - non-steroidal anti-inflammatory drugs (NSAIDS), such as ibuprofen can reduce pain and swelling. If you suffer from asthma, kidney disease or liver disease do not take NSAIDs without first checking with your doctor. Steroid injections, these can reduce tendon swelling, but should be performed with caution, as this process has been associated with a greater risk of tendon rupture. A doctor would likely perform the injection while scanning the area with ultrasound to reduce this risk. Compression bandages and orthotic devices, such as ankle supports and shoe inserts can aid recovery as they take the stress off the Achilles tendon.
Surgical Treatment
Percutaneous Achilles Tendon Surgery. During this procedure the surgeon will make 3 to 4 incisions (approx. 2.5 cm long) on both sides of the Achilles tendon. Small forceps are used to free the tendon sheath (the soft tissue casing around your Achilles tendon) to make room for the surgeon to stitch/suture any tears. Skilled surgeons may perform a percutaneous achilles tendon surgery with ultrasound imaging techniques to allow for blink suturing with stab incisions made by a surgical suture needle. This procedure can be done in 3 different ways depending on the preference and experience of your surgeon. Instead of making several 2.5 cm incisions for this procedure, some surgeons will use guided imaging with an ultrasound to see the Achilles tendon tissue without having to open up your ankle. For this technique, they will use a surgical needle to repeatedly stab your Achilles tendon. These "stab incisions" will allow the surgeon to "blindly" suture your tendon without seeing the actual tissue. As another option - some surgeons will only make 1 to 3 incisions for smaller surgical implements to repair your tendon while relying on imaging ultrasound to see your damaged tissue. During either procedure the use of ultrasound imaging or endoscopic techniques requires a very skilled surgeon.
Prevention
By properly training the body, an athlete can build the strength of their tendons and muscles. Following a workout and dieting plan, the body will be able to build muscle and strengthen most effectively. Additionally, doing the following can prevent tendinitis. Wearing appropriate shoes will give your foot the support it needs for proper movements of the foot and ankle. Improper movements will put additional stress on your body. Stretching before an athletic activity, Stretching primes the body for a taxing activity. Additionally, this will get your blood flowing and reduce the risk of pulling a muscle. Ask your doctor about orthotics, Custom orthotics can help get your foot into proper alignment. If the foot does not execute proper mechanics, the body will adjust which will cause pain and increase the chances of injury.
What Will Cause Heel Discomfort And The Ways To Remedy It

Overview
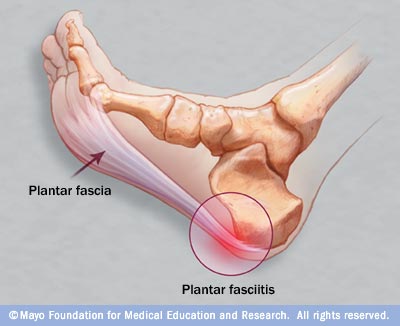
Plantar fasciosis is a foot condition characterized by heel pain and pain in your plantar fascia-a strong and dense connective tissue structure on the sole of your foot that supports your foot arch. This condition has historically been called plantar fasciitis because it was believed that plantar fascia inflammation was the principle underlying cause. Plantar fasciosis is a more accurate name for this condition because it involves degeneration-microtears, cell death-of your plantar fascia, not inflammation. Active men between the ages of 40 and 70 are most commonly affected by this health problem.
Causes
It usually starts following an increase in activity levels. Increase in weight. Standing for long periods. Poor footwear. Tight muscle groups. Abnormal pressure on the plantar Fascia can be caused by any of the above. The plantar fascia becomes inflamed and tiny rips can occur where it attaches into the inside of the heel bone. The area becomes inflamed and swollen, and it is the increase in fluid to the area that accumulates when weight is taken off the area that then causes the pain on standing.
Symptoms
A sharp pain in the center of your heel will most likely be one of the biggest symptoms of plantar fasciitis. A classic sign of plantar fasciitis is when the pain is worst during the first steps you take in the morning.
Diagnosis
During the physical exam, your doctor checks for points of tenderness in your foot. The location of your pain can help determine its cause. Usually no tests are necessary. The diagnosis is made based on the history and physical examination. Occasionally your doctor may suggest an X-ray or magnetic resonance imaging (MRI) to make sure your pain isn't being caused by another problem, such as a stress fracture or a pinched nerve. Sometimes an X-ray shows a spur of bone projecting forward from the heel bone. In the past, these bone spurs were often blamed for heel pain and removed surgically. But many people who have bone spurs on their heels have no heel pain.
Non Surgical Treatment
Treatment for heel pain usually involves using a combination of techniques, such as stretches and painkillers, to relieve pain and speed up recovery. Most cases of heel pain get better within 12 months. Surgery may be recommended as a last resort if your symptoms don't improve after this time. Only 1 in 20 people with heel pain will need surgery. Whenever possible, rest the affected foot by not walking long distances and standing for long periods. However, you should regularly stretch your feet and calves using exercises such as those described below. Pain relief. Non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, can be used to help relieve pain. Some people also find applying an ice pack to the affected heel for 5-10 minutes can help relieve pain and inflammation. However, do not apply an ice pack directly to your skin. Instead, wrap it in a towel. If you do not have an ice pack, you can use a packet of frozen vegetables.
Surgical Treatment
Surgery may be considered in very difficult cases. Surgery is usually only advised if your pain has not eased after 12 months despite other treatments. The operation involves separating your plantar fascia from where it connects to the bone; this is called a plantar fascia release. It may also involve removal of a spur on the calcaneum if one is present. Surgery is not always successful. It can cause complications in some people so it should be considered as a last resort. Complications may include infection, increased pain, injury to nearby nerves, or rupture of the plantar fascia.
Prevention
While there are no sure ways to prevent plantar fasciitis, these prevention tips may be helpful. Keep your weight under reasonable control. Wear comfortable, supportive shoes. Use care when starting or intensifying exercise programmes.
What Is Heel Discomfort
Overview
Plantar Fasciitis is actually, in most cases, plantar fasciosis but it’s a bit like pen/biro or hoover/vacuum. The term ‘-itis‘ means ‘inflammation’. This is a term we use for this problem in the early stages of damage because it usually is quite literally an inflammation of part of the plantar fascia. So, what is commonly known as ‘plantar fasciitis’ is really ‘plantar fasciosis’ - a degradation or degeneration of the collagen fibres because of prolonged (most of your adult life) unsustainable stress being applied to the fascia. So, we call it plantar fasciitis but it usually hasn’t been an ‘-itis‘ for years and that is why in many cases anti-inflammatory drugs do not help ease the pain of walking. This is also why most sufferers experience pain first thing in the morning. If inflammation was the source of discomfort then why would it hurt after a nights rest and the good old drugs pumping through your system.
Causes
Although plantar fasciitis may result from a variety of factors, such as repeat hill workouts and/or tight calves, many sports specialists claim the most common cause for plantar fasciitis is fallen arches. The theory is that excessive lowering of the arch in flat-footed runners increases tension in the plantar fascia and overloads the attachment of the plantar fascia on the heel bone (i.e., the calcaneus). Over time, the repeated pulling of the plantar fascia associated with excessive arch lowering is thought to lead to chronic pain and inflammation at the plantar fascia’s attachment to the heel. In fact, the increased tension on the heel was believed to be so great that it was thought to eventually result in the formation of a heel spur.
Symptoms
The pain associated with plantar fasciitis is typically gradual in onset and is usually located over the inner or medial aspect of the heel. Occasionally, the pain will be sudden in onset, occurring after missing a step or after jumping from a height. The pain is commonly most severe upon arising from bed in the morning, or after periods of inactivity during the day. Thus, it causes what is known as "first-step pain." The degree of discomfort can sometimes lessen with activity during the course of the day or after "warming-up", but can become worse if prolonged or vigorous activity is undertaken. The pain is also often noted to be more severe in bare feet or in shoes with minimal or no padding at the sole.
Diagnosis
After you describe your symptoms and discuss your concerns, your doctor will examine your foot. Your doctor will look for these signs. A high arch, an area of maximum tenderness on the bottom of your foot, just in front of your heel bone. Pain that gets worse when you flex your foot and the doctor pushes on the plantar fascia. The pain improves when you point your toes down. Limited "up" motion of your ankle. Your doctor may order imaging tests to help make sure your heel pain is caused by plantar fasciitis and not another problem. X-rays provide clear images of bones. They are useful in ruling out other causes of heel pain, such as fractures or arthritis. Heel spurs can be seen on an x-ray. Other imaging tests, such as magnetic resonance imaging (MRI) and ultrasound, are not routinely used to diagnose plantar fasciitis. They are rarely ordered. An MRI scan may be used if the heel pain is not relieved by initial treatment methods.
Non Surgical Treatment
More than 90% of patients with plantar fasciitis will improve within 10 months of starting simple treatment methods. Rest. Decreasing or even stopping the activities that make the pain worse is the first step in reducing the pain. You may need to stop athletic activities where your feet pound on hard surfaces (for example, running or step aerobics). Ice. Rolling your foot over a cold water bottle or ice for 20 minutes is effective. This can be done 3 to 4 times a day. Nonsteroidal anti-inflammatory medication. Drugs such as ibuprofen or naproxen reduce pain and inflammation. Using the medication for more than 1 month should be reviewed with your primary care doctor. Exercise. Plantar fasciitis is aggravated by tight muscles in your feet and calves. Stretching your calves and plantar fascia is the most effective way to relieve the pain that comes with this condition. Cortisone injections. Cortisone, a type of steroid, is a powerful anti-inflammatory medication. It can be injected into the plantar fascia to reduce inflammation and pain. Your doctor may limit your injections. Multiple steroid injections can cause the plantar fascia to rupture (tear), which can lead to a flat foot and chronic pain. Soft heel pads can provide extra support. Supportive shoes and orthotics. Shoes with thick soles and extra cushioning can reduce pain with standing and walking. As you step and your heel strikes the ground, a significant amount of tension is placed on the fascia, which causes microtrauma (tiny tears in the tissue). A cushioned shoe or insert reduces this tension and the microtrauma that occurs with every step. Soft silicone heel pads are inexpensive and work by elevating and cushioning your heel. Pre-made or custom orthotics (shoe inserts) are also helpful. Night splints. Most people sleep with their feet pointed down. This relaxes the plantar fascia and is one of the reasons for morning heel pain. A night splint stretches the plantar fascia while you sleep. Although it can be difficult to sleep with, a night splint is very effective and does not have to be used once the pain is gone. Physical therapy. Your doctor may suggest that you work with a physical therapist on an exercise program that focuses on stretching your calf muscles and plantar fascia. In addition to exercises like the ones mentioned above, a physical therapy program may involve specialized ice treatments, massage, and medication to decrease inflammation around the plantar fascia. Extracorporeal shockwave therapy (ESWT). During this procedure, high-energy shockwave impulses stimulate the healing process in damaged plantar fascia tissue. ESWT has not shown consistent results and, therefore, is not commonly performed. ESWT is noninvasive-it does not require a surgical incision. Because of the minimal risk involved, ESWT is sometimes tried before surgery is considered.

Surgical Treatment
Most patients have good results from surgery. However, because surgery can result in chronic pain and dissatisfaction, it is recommended only after all nonsurgical measures have been exhausted. The most common complications of release surgery include incomplete relief of pain and nerve damage.
Stretching Exercises
Stretching your plantar fasciitis is something you can do at home to relieve pain and speed healing. Ice massage performed three to four times per day in 15 to 20 minute intervals is also something you can do to reduce inflammation and pain. Placing arch supports in your shoes absorbs shock and takes pressure off the plantar fascia.